Introduction
The end of the Covid-19 pandemic now seems much closer than it did even six months ago with large-scale vaccination efforts taking place across the world. Countries are racing to vaccinate their residents to achieve “herd” immunity and move on to what may be considered our “new” normal. With the pandemic claiming more than 3.3 million[i] lives globally, vaccines are being used to save lives and limit future deaths. However, it may be worth nothing that some of the preventative methods that were utilized – like mask mandates and stay-at-home  orders – have also saved lives. Therefore, this research seeks to understand if mask mandates and stay-at -home orders had any effect on vaccination rates. That is: can preventive orders issued early on in the pandemic be used to estimate state vaccination rates? In order to understand if early interventions such as mask mandates and stay-at-home orders are indicative of higher vaccination rates multiple regression models were run. Several other key variables are also analyzed to understand their effects on vaccination rates. After conducting an analysis of the data several considerations are put forward about how to address vaccine disparities. Some of the included suggestions include providing education about the vaccine and working together with trusted community members.
orders – have also saved lives. Therefore, this research seeks to understand if mask mandates and stay-at -home orders had any effect on vaccination rates. That is: can preventive orders issued early on in the pandemic be used to estimate state vaccination rates? In order to understand if early interventions such as mask mandates and stay-at-home orders are indicative of higher vaccination rates multiple regression models were run. Several other key variables are also analyzed to understand their effects on vaccination rates. After conducting an analysis of the data several considerations are put forward about how to address vaccine disparities. Some of the included suggestions include providing education about the vaccine and working together with trusted community members.
Methodology
The data used in this state-level analysis came from several places. All of the vaccination data came from the CDC Covid-19 Vaccination Dashboard Tracker[ii]. Information regarding mask mandates and stay-at-home orders came from the Raifman J. Et. Al Covid-19 US State Policy (CUSP) database[iii]. Information from the CUSP database around stay-at-home orders and mask mandates was coded for specific dates when the orders took effect. This data was transformed into two “dummy” variables indicating whether or not a state had stay-at-home orders and if they had mask mandates during the pandemic. A “dummy” variable is used in regression models to indicate binary responses such as “yes” or “no”. In this case it was used to indicate whether or not a state had one of the aforementioned policies in place. Creating a “dummy” variable allows us to compare states that had these preventative measures in place and those that did not. Population estimates for those 18+, 65 and over, and state population came from the 2019 census[iv]. Racial minority population estimates were also taken from 2019 census data. Estimates of health care spending were taken from the Kaiser Family Foundation[v] and transformed to showcase per capita health care spending in each state. Voter share information was taken from a Cook Political voter tracker for the 2020 presidential election.[vi] The goal of this model is to examine if there was any variation in vaccination rates when the coronavirus vaccination first hit the market. We also examined if early preventative measures were any indicator of Covid-19 vaccination rates. The rationale behind this approach was the thinking that states which took action against the virus would be better prepared to vaccinate their constituents. The data looks at vaccination rates across the United States on May 6, 2021. The next section of this research discusses key findings from regression models and summary statistics that were analyzed.
Analysis
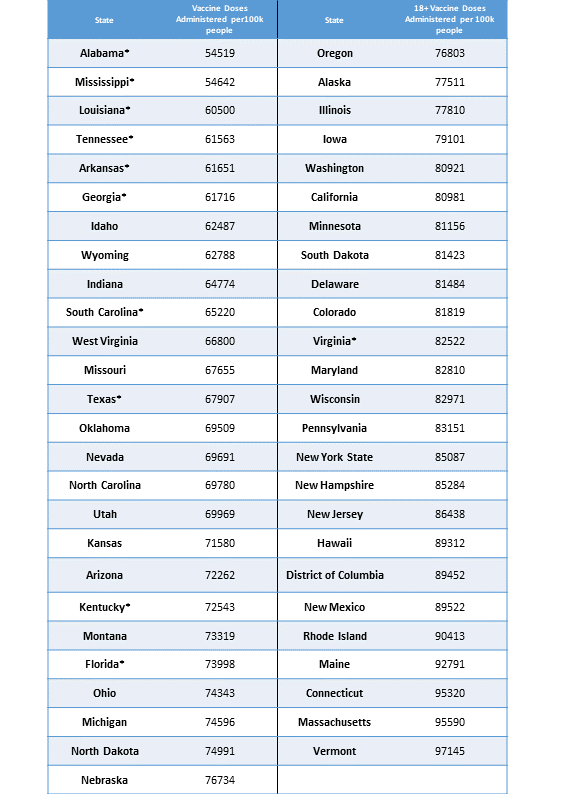
Summary statistics for vaccines administered per 100,000 people for those 18 and over are displayed in the appendix for May 6. We are looking at doses administered in doses per 100,000 to standardize vaccination rates across states of various sizes. Based on this metric, Vermont has the highest vaccination rate per 100,000 18 plus adults with 97,145 doses being administered as of May 6. Alabama ranked at the bottom of the list with 54,519 doses per 100,000 18 plus adults while Michigan was ranked 28th with 74,596 doses administered per 100,000 18 plus adults. This shows that there is some variation in state vaccination rates, and this is shown in the summary statistics listed in the appendix.
When looking at our two key explanatory variables – stay-at-home orders and mask mandates – we can note that an overwhelming majority of states adopted both practices at some point during the pandemic. Eighty percent of states have implemented some sort of mask mandates while 78% of states have issued stay-at-home orders. To help account for more variation in the data our models also controlled for the percentage of the population representing minorities, percentage of the state that voted for President Trump in the 2020 election, and whether or not a state was located in the south of the U.S. The south variable was constructed based on states that were in the Confederacy. States included in the south variable have an asterisk by their name in the doses administered per 100,000 18-plus adults’ chart as it is included in the appendix. The percentage of Republicans in a state is measured by examining the share of people who voted for Trump in the 2020 election cycle. These variables offered valuable information about variation at the state level. Several models were examined; only three will be discussed in this section.
The first model looks at vaccination rates in states that have enacted mask mandates at any time during the pandemic. States with mask mandates were found to have vaccination rates that were 9,148 doses higher per 100,000 compared to states that did not have mask mandates. This is statistically significant at the 1% level and practically significant as this is more than half a standard deviation. The next model examines the impact of adding stay-at-home orders to our original model. Stay-at-home orders and mask mandates are included to address the intent to slow the spread of the virus by state policy makers. The assumption is states that have these orders are taking stricter action to combat the virus. In this model, our variable for stay-at-home orders is not statistically nor practically significant because the chance of seeing a value like this is higher than 10%. The difference between states without stay-at-home orders was roughly 13 doses less per 100,000 18 plus adults. The statistical and practical significance is unchanged for the mask mandate variable as vaccine administration rates only dropped by 2 vaccinations per 100,000 18 plus adults and it is still significant at the 1% level.
The last model we are going to examine has controls for the share of a state’s Republican voters who voted for Trump in the 2020 election, the percentage of racial minorities in a state, and if the state is in the south. This model estimates statistical significance for stay-at-home orders, the share of Republican voters, and southern states at the 1% level. The variables for the share of Republicans and minorities was centered around their respective means and allows us to estimate the impact on changes relative to their mean values. A one percentage point increase in the share of Republicans above the mean -- holding all else equal -- is associated with a 78,616 decrease in vaccination rates per 100,000 18 plus adults. This would mean that states with more Republican voters than the average would be expected to have lower vaccination rates. States that issued stay-at-home orders during the pandemic -- holding all else equal -- in our model are expected to have 7,405 fewer vaccines administered per 100,000 18 plus adults than states that didn’t. It is worth noting that 40 states had stay-at-home orders and this model does not differentiate when these orders were issued. This means that states that issued stay-at-home orders late into the pandemic and states that issued them earlier are included in this variable. Finally, states in the south are expected to have vaccine administration rates that are 10,351 doses lower per 100,000 18 plus adults than states not in the south. This is statistically significant and almost a full standard deviation change. This information shows us that not only is early intervention important for current vaccination rates, but also the region of the country where citizens are located in and the share of Republican voters in a state is important as well.
Considerations
As mentioned, this data was gathered May 6, 2021 and at that point in time the vaccine was available for all U.S. adults. Vaccine disparities have appeared between groups of Americans as more analysis has been done at the county level[vii]. Specifically, black and brown communities were being vaccinated at lower rates than their white counterparts. This may not show up in some state-level analysis for a few reasons. Initially, demographic information wasn’t collected for those obtaining vaccinations. That meant this inequity couldn’t be seen in the data initially. This difference in vaccination rates for communities of color could also be misrepresented at the state level because counties with higher vaccination rates could be skewing the data at the state level. By understanding differences in vaccination rates at the county level, strategies can be developed to increase county vaccination rates. This would allow states to move closer to achieving herd immunity to the coronavirus. Herd immunity levels are estimated to be around 70%[viii] and the U.S. has a current vaccination rate around 48.4% for adults 18 and over who are fully vaccinated as of May 20 2021[ix]. This number needs to increase in order for the U.S. to move forward from this pandemic. One way to increase this number is to focus on people who have not yet received the vaccine. Specifically focusing on those who are hesitant to receive the coronavirus vaccination.
A key component of this effort would be to mobilize those who[x] are still hesitant to receive the vaccine. There are several key things that the U.S. can do at the federal level to help incentivize those who are unsure about obtaining the Covid-19 vaccine. Federal guidance could give states valuation information leading them to increase their own vaccination rates.
First, health officials can work to provide more accessible information to the general public. The coronavirus pandemic is still rapidly changing, and we are learning more about how different variants of the virus react to the vaccine. Providing easily understood information about the vaccine is one way to help shift the perception about its safety. Making sure that citizens understand how vaccines work and are approved could increase their willingness to obtain the vaccine to prevent the COVID-19 virus.
Next, individuals can work to educate and persuade those around them who are “on the fence” about the Covid-19 vaccine. Those who are hesitant to obtain the vaccine could slow down the race toward herd immunity. This behavior makes it more difficult for the country to safely get back to business, education, social relationships, economic development – in other words, the activities of a world not kept home in fear of disease as the virus will have more susceptible host to infect. Working to educate and persuade people on the fence – or divided about the vaccine – is one way to increase vaccination rates[xi]. By focusing on those who are on the fence and not those who are fully against vaccinations we utilize our resources in the most efficient way. Also, by having those close to them engage in these conversations there may be a sense of trust that allows them to get through to those individuals.
Lastly, working to ensure that there is an equitable vaccine rollout in the U.S. could set the for equitable rollout throughout the world. Current research indicates that there are significant differences between vaccine distribution within the U.S. and throughout the globe. According to Anna R. et al, it is estimated that wealthy countries have purchased more than half the shares of the coronavirus vaccines even though they represent only 19% of the adult population in the world[xii]. This could lead to these countries facing higher infection rates, which would eventually result in an overwhelmed healthcare system and ultimately more deaths. The aforementioned are all things that could be avoided with more equitable vaccine distribution plans. By working to close this gap internationally and support parts of the world that are being decimated by the pandemic, we can work towards a better tomorrow that includes better health outcomes, revitalized economies, and the decline of Covid-19 cases.
Limitations
This research only examines overall vaccination rates on May 6 at the state level. It does not account for daily variation in vaccine administration rates. Future research may benefit from looking at vaccination rates across time on a weekly or daily basis to get a better sense of vaccine variation in the U.S. Vaccine administration could also be examined during key periods such as before Johnson & Johnson received Emergency Use Authorization (EUA) from the FDA[xiii] and after requirements regarding age, health, and employment for vaccinations were eased in various states. Examining specific state variation in vaccine rates could also provide useful insight into vaccine inequity. Researchers could also benefit from grouping state responses together based on their timing of when they responded to the pandemic. States that delayed action and states that took earlier action could have differences in vaccination rates based on the timeliness of the state’s response to the pandemic. By grouping these states together, a more nuanced regression model could be produced. This would allow researchers to examine which specific populations are underserved within the various states and potentially make it easier/more efficient to craft a strategy addressing inequity. A growing body of research suggests inequity – meaning that poorer, older, younger, rural, urban populations – are being ignored by current vaccine distribution and practices. By attempting to increase vaccination rates in a coordinated and equitable way we can move forward toward a new normal that includes students returning to the classroom, the return of in-person sporting events, and safe international trips.
Bibliography
Bureau, US Census. “State Population by Characteristics: 2010-2019.” The United States Census Bureau, https://www.census.gov/data/tables/time-series/demo/popest/2010s-state-detail.html. Accessed 5 May 2021.
CDC. “COVID Data Tracker.” Centers for Disease Control and Prevention, 28 Mar. 2020, https://covid.cdc.gov/covid-data-tracker.
Commissioner, Office of the. “Janssen COVID-19 Vaccine.” FDA, FDA, May 2021. www.fda.gov, https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/janssen-covid-19-vaccine.
D’Souza, Gypsyamber, and David Dowdy. “What Is Herd Immunity and How Can We Achieve It With COVID-19?” Johns Hopkins Bloomberg School of Public Health, https://www.jhsph.edu/covid-19/articles/achieving-herd-immunity-with-covid19.html. Accessed 16 May 2021.
“Health Care Expenditures by State of Residence (in Millions).” KFF, 16 June 2017, https://www.kff.org/other/state-indicator/health-care-expenditures-by-state-of-residence-in-millions/.
Khubchandani, Jagdish et al. “COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment.” Journal of community health vol. 46,2 (2021): 270-277. doi:10.1007/s10900-020-00958-x
Lassman, David, et al. “Health Spending By State 1991–2014: Measuring Per Capita Spending By Payers And Programs.” Health Affairs, vol. 36, no. 7, July 2017, pp. 1318–27. DOI.org (Crossref), doi:10.1377/hlthaff.2017.0416.
Ndugga, Nambi, et al. “How Are States Addressing Racial Equity in COVID-19 Vaccine Efforts?” KFF, 10 Mar. 2021, https://www.kff.org/racial-equity-and-health-policy/issue-brief/how-are-states-addressing-racial-equity-in-covid-19-vaccine-efforts/.
Raifman J, Nocka K, Jones D, Bor J, Lipson S, Jay J, and Chan P. (2020). "COVID-19 US state policy database.”
Rouw, Anna, et al. “Global COVID-19 Vaccine Access: A Snapshot of Inequality.” KFF, 17 Mar. 2021, https://www.kff.org/policy-watch/global-covid-19-vaccine-access-snapshot-of-inequality/.
U.S. Census Bureau; American Community Survey, 2019 American Community Survey 1-Year Estimates, Table CP05; generated by Roderick Bullard; using data.census.gov; <https://data.census.gov/cedsci/>; (17 May 2021).
Wagner, Abram, and Trina Shanks. Vaccine Hesitancy and COVID-19 | News Center | University of Michigan School of Public Health | Coronavirus | Epidemiology | Health Disparities | Health Communication | Infectious Disease | Urban Health | Health Care Access | Detroit | Racism | Vaccines. https://sph.umich.edu/news/2021posts/vaccine-hesitancy-and-covid-19.html. Accessed 5 May 2021.
Wasserman, David, et al. “2020 Popular Vote Tracker.” The Cook Political Report, https://cookpolitical.com/2020-national-popular-vote-tracker. Accessed 17 May 2021.
WHO COVID-19 Dashboard. Geneva: World Health Organization, 2020. Available online: https://covid19.who.int/ (last cited: [17 May 2021]).
Appendix
Summary Statistics
|
Variable |
Obs |
Mean |
Std. Dev. |
Min |
Max |
|
DosesAd~100K |
51 |
96500.41 |
12165.42 |
69684 |
117733 |
|
Stayathome |
51 |
.7843137 |
.4153902 |
0 |
1 |
|
Maskmandate |
51 |
.8039216 |
.4009792 |
0 |
1 |
|
Republican~e |
51 |
.4921509 |
.1199358 |
.0539732 |
.6993623 |
|
Racialmino~n |
51 |
.324451 |
.1623092 |
.071 |
.785 |
|
republican~d |
51 |
.0021509 |
.1199358 |
-.4360268 |
.2093623 |
Regression Models

State Vaccination Rates
[xiii] https://www.fda.gov/emergency-preparedness-and-response/coronavirus-dise...
Roderick Bullard is a Masters of Public Policy student who obtained his undergraduate degree in psychology and criminal justice at Michigan State University in 2020. He is an IPPSR Graduate Fellow. His policy interests revolve around mental health and wellness, criminal justice reform and social justice.



